About this course:
This learning module reviews relevant terminology and explores current research on best practices and related wound care for pressure injuries caused by medical devices or hospitalization
Course preview
This learning module reviews relevant terminology and explores current research on best practices and related wound care for pressure injuries caused by medical devices or hospitalization.
After this learning module, the learner will be prepared to:
define the incidence and prevalence of pressure injuries from hospitalization
review the pathophysiology of the skin related to the incidence of pressure injuries
understand pressure injury risk from medical device use
discuss the impact of hospitalization on pressure injury risk
explore national patient safety goals related to pressure injuries
describe the management of pressure injuries based on current clinical guidelines
Pressure injuries are localized damaged skin and soft tissue areas caused by unrelieved pressure, friction, shearing, and moisture. They often result from immobility or the use of a medical device. Pressure injuries continue to be a significant problem in acute care hospitals and long-term care facilities. Each year more than 2.5 million patients in the US are affected by hospital-acquired pressure injuries (HAPIs), formerly described as pressure ulcers or pressure sores, resulting in 60,000 deaths. Treating a single full-thickness pressure injury can cost over $70,000, resulting in a combined $11 billion annually in the US alone. A HAPI can result in significant patient harm, including costly treatments, increased pain, extended hospitalization, and increased morbidity and mortality. Between 2014 and 2017, the incidence of HAPIs decreased by 13%; however, since 2017, there has been a 6% increase in the incidence (California Hospital Patient Safety Organization [CHPSO], 2017; Mondragon & Zito, 2021; The Joint Commission, 2022b).
Up to 15% of patients admitted to the hospital will develop a pressure injury in the US. The prevalence of pressure injuries is higher in long-term and critical care settings. The Centers for Medicare and Medicaid Services (CMS) denies all payments, or reimbursements, for HAPIs classified as stage III or IV. CMS has deemed these stages of pressure injury preventable and classifies them as never events. In addition to paying or reimbursing 0% for the treatment of these pressure Injuries, CMS can also penalize hospitals with a 1% reduction in overall reimbursement for having an elevated HAPI rate if the hospital's HAPI rate falls into the bottom 25% of hospitals nationwide (Black & Maegley, 2019; CMS, 2021; Mondragon & Zito, 2021).
Anatomy and Physiology of the Skin
The skin covers the entire body and is the largest organ, accounting for approximately 20% of total body weight. The skin's primary function is to protect the internal organs and structures from biological invasion, ultraviolet radiation, fluid loss, and physical damage. Additional skin functions are providing thermoregulation through sweating and blood flow regulation, synthesizing vitamin D, relaying sensation from nerve endings, excreting salts and small amounts of waste products, and providing aesthetics and communication. The skin comprises the outer layer or epidermis, the deeper layer or dermis, and the subcutaneous layer or hypodermis (see Figure 1 below). The skin's health influences overall health and has a profound psychological significance since it identifies the individual with unique facial and body characteristics. Self-image may be enhanced or deterred by society's standards for one's appearance (McCance & Huether, 2019). 
The epidermis acts as a defensive barrier that constantly renews itself by shedding the superficial layer (stratum corneum). It is composed primarily of keratinocytes embedded in a lipid matrix. The epidermis is slightly acidic with a pH of 4.5-6 and comprises five layers, the stratum corneum, stratum lucidum, stratum granulosum, stratum spinosum, and stratum basale. Each layer has a specific function and plays a role in the healing process of wounds (McCance & Huether, 2019).
The stratum corneum is composed of tough superficial sheets of cornified cells.
...purchase below to continue the course
The dermis is the next layer below the epidermis. It is 1-4 mm thick and composed of three types of connective tissue: collagen, elastin, reticulin, and a gel-like ground substance. The primary role of the dermis is to support and provide nutrition to the epidermis. This layer consists primarily of connective tissue or collagen, a tough, fibrous protein that helps skin resist tearing. The dermis is resilient and elastic to allow the skin to stretch with body movement. The dermis houses the nerves, sensory receptors, blood vessels, and lymphatics. The hair follicles, sebaceous glands, and sweat glands are also embedded in the dermis (McCance & Huether, 2019).
The third layer of skin is the hypodermis or subcutaneous tissue. This layer connects the dermis to the underlying muscle. This layer comprises blood vessels, adipose tissue, and connective tissue that support the dermis. Macrophages, fibroblasts, nerves, and hair follicle roots are also found within this layer. The fat stored in this layer provides internal structures with additional protection and insulation against the cold (McCance & Huether, 2019).
Pathophysiology
Pressure injuries are formed when the pressure applied to the skin and soft tissues is above a certain threshold for a prolonged period. This prolonged pressure leads to tissue ischemia and eventually necrosis due to disruption of venous and arterial blood flow. This disruption in blood flow impairs the delivery of nutrients and the removal of metabolic waste products. This accumulation of waste products creates an acidic environment, leading to cellular death and tissue damage. While the skin and underlying muscle can withstand pressure for brief periods, even slight sustained pressure can lead to these injuries. This pressure can be caused by the patient's body weight or an external force, such as a medical device. The compression from mattresses, wheelchair pads, bed rails, or other surfaces found in the patient's environment serves as the source of this pressure. Shearing forces against the tissues also cause injuries that extend deep into the skin's layers. Maceration from prolonged exposure to moisture due to incontinence or diaphoresis can expose the skin to further damage from friction, shearing, or pressure. Reperfusion of an area with limited blood flow for an extended time can also cause injury due to the inflammatory response. These injuries usually occur over a bony prominence such as the sacrum, heels, ischia, and greater trochanters (see Figure 2 below). Approximately 70% of pressure injuries appear on the hips or buttocks, with 15-25% on the malleolar, heel, patellar, and pretibial areas. Other areas at risk for pressure injuries include the scapula, elbow, and occipital region (Kirman, 2020; McCance & Huether, 2019; Mondragon & Zito, 2021; National Pressure Injury Advisory Panel [NPIAP], 2019). 
While the skin is visible during an inspection, the underlying muscle tissue is damaged first in pressure injuries. Muscle tissue requires increased oxygen and nutrients when compared to surface tissues. Only two hours of continuous pressure can damage the underlying muscle and tissue, creating a wound in the shape of an inverted cone from the surface down to the muscle. Individuals with darker pigmented skin are at a higher risk of pressure injuries due to less visible early signs of skin damage (Kirman, 2020; McCance & Huether, 2019).
Staging Pressure Injuries
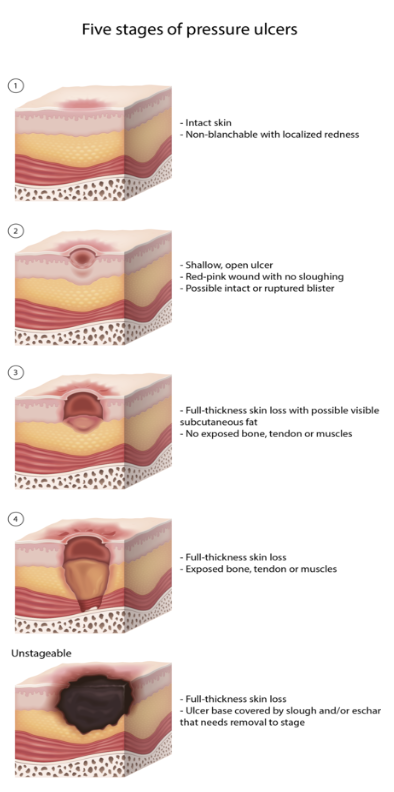
The NPIAP updated its staging system for pressure inures in 2016 (see Figures 3 and Table 1 below). The system includes four main stages of pressure injury ranging from I to IV. Pressure injuries can only be numerically staged if the tissue injury can be visualized or palpated. The NPIAP added unstageable pressure and deep tissue injuries to describe injuries that cannot be visualized due to slough, eschar, or color changes. Once deep tissue injuries evolve, or an unstageable pressure injury is debrided, the injury can be staged on the numeric scale. The stages are not considered progressive (either backward or forward), and downstaging is not recommended. The system is used to describe a wound at a specific assessment time and is meant to be used as a communication tool among healthcare providers and various disciplines to drive the plan of care (NPIAP, 2019).


The NPIAP (2019) also addresses the staging of medical device-related pressure injuries (MDRPIs) and mucosal membrane pressure injuries (see Table 2 below).  Risk Factors
Risk Factors
General
The literature has identified over 100 factors increasing the risk of a HAPI, but the most cited risk is patient immobility. Any patient can develop a HAPI, but their incidence is higher in unique populations, including patients receiving palliative care, those with spinal cord injuries, neonates and children, and individuals in critical condition. HAPIs are also highest in patients in critical care and long-term care settings (NPIAP, 2019; Schub & Smith, 2021). Other leading risk factors include the following:
decreased activity level
changes in sensory perception
frailty
being overweight or underweight
malnutrition
an extended stay in a healthcare facility
immunodeficiency
incontinence
edema
smoking
diabetes mellitus
hip fracture
stroke
renal failure (Kim et al., 2022; NPIAP, 2019; Schub & Smith, 2021)
Elderly patients have the highest rate of pressure injuries. Although advanced age alone is a contributing factor, the risk increases with co-morbidities such as decreased mobility and activity level, impaired skin status, decreased oxygenation and perfusion, or increased skin moisture. Patients with mobility limitations, especially those confined to a bed or chair, have a higher risk of pressure injury development (NPIAP, 2019). Available risk tools examine contributing factors, including but not limited to:
mobility and activity related to activities of daily living (ADLs)
activity descriptors such as chairfast or bedfast
factors affecting mobility, including weakness or paralysis
increased friction or shear due to the inability to reposition (NPIAP, 2019)
Perfusion and oxygenation directly relate to the risk of developing a pressure injury. Vascular disease, hypertension (HTN), diabetes, smoking, and edema cause decreased circulation to the skin and increase the risk of tissue ischemia leading to injury and reduced healing. Skin moisture is a risk factor for pressure injury development across the literature. While a certain amount of hydration is necessary for skin condition and function, excess moisture increases skin vulnerability by affecting the skin's mechanical properties and barrier function. Factors that increase the risk include diaphoresis and fecal or urinary incontinence. Nutritional deficits are associated with altered skin tolerance, morphology of the tissues, physiology, ability for repair, and thermal properties. Each of these factors can increase the risk of pressure injury (NPIAP, 2019). Specific risk factors to assess include:
food intake descriptors
low weight or recent weight loss
low or high body mass index (BMI)
malnutrition
decreased or increased mid-arm circumference (MAC; NPIAP, 2019)
Decreased sensory perception occurs with spinal cord injuries or other neurological disorders. Like the elderly patient, these individuals have the highest risk when co-morbidities exist. Co-existing factors such as loss of sensation, immobility, and altered pathophysiology increase the likelihood of pressure injuries in these patients. Altered hematological values of particular concern include lymphocytopenia, hypoalbuminemia, anemia, or an elevated C-reactive protein. Additional concerns are urea and electrolyte imbalances. A creatinine level above 1 mg/dL is associated with a higher risk of pressure injury development. An increase or significant decrease in body temperature can lead to an increased risk for injury to the skin as it affects its susceptibility and tolerance. A patient with sustained fever or hypothermia is at an increased risk of developing a HAPI. Finally, poor mental or physical health can lead to pressure injury (NPIAP, 2019). Risk factors in this category include:
chronic wounds
medication use
chronic illnesses including AIDS, diabetes, or respiratory conditions
mental health conditions, including dementia
acute injuries
surgical recovery
extended hospitalizations (NPIAP, 2019)
Medical Device Risk Factors
In 2016 the NPIAP redefined pressure injuries and included medical devices as a source of pressure injuries. An MDRP is a pressure injury that results from using a device designed and applied for diagnostic or therapeutic purposes. Medical devices are an integral part of treating patients in the acute care setting. Nearly all hospitalized patients require at least one medical device, which increases the risk of injury. Patients in the critical care setting have an even higher risk of developing an MDRPI due to the increased number of medical devices needed to treat these patients. Approximately 33% of all pressure injuries result from medical device use. The wound typically takes on the pattern or shape of the offending medical device and should be staged using the NPIAP staging system (see Table 5). Poorly fitting or improperly positioned fixation devices used to secure a medical device can render the patient vulnerable to an MDRPI. Many MDRPIs are included in reports related to the specific device rather than in pressure injury reports; thus, the number of MDRPIs may be far higher than is currently thought. These injuries are harder to determine risk for as well. While the skin assessment tools may be predictive of pressure injuries, they may not be predictive of MDRPIs (Camacho-Del Rio, 2018; Jackson et al., 2019; NPIAP, n.d.; Weber et al., 2021).
Like the general risk factors listed above, the risk factors for MDRPIs include impaired sensation, poor perfusion, altered tissue tolerance, poor nutritional status, or moisture under the device (The Joint Commission, 2018). Medical devices associated with pressure injuries include, but are not limited to, the following:
enteral feeding tubes
oxygen delivery systems (nasal cannula, continuous positive airway pressure (CPAP), bilevel positive airway pressure (BiPAP), non-rebreather, endotracheal tube)
pulse oximeters
intravenous catheters (arterial and venous)
indwelling urinary catheters
orthopedic devices (including braces and casts)
cervical collars
restraints
negative pressure wound vacs
tracheostomy ties or securement devices
sequential compression devices
TED hose or compression stockings
abdominal binders (Camacho-Del Rio, 2018; The Joint Commission, 2018; Weber et al., 2021)
Patient-specific risk factors for developing an MDRPI from one of the previously listed medical devices include:
extended length of stay (LOS)
receiving vasopressors
low Braden Scale score
dependent on mechanical ventilation
advanced age
concurrent HAPI not attributable to a medical device
receiving enteral nutrition
critically ill (Weaver et al., 2021)
MDRPIs can occur in any area within the hospital: acute care, transitional care, critical care, pediatrics, trauma, and rehabilitation units. Since there is a significant risk for MDRPIs among many patient populations, the nurse's clinical judgment and visual inspection are vital to protect patients. Policies and procedures focusing on the increased assessment of the medical device location are needed to prevent MDRPIs. Early intervention with repositioning the device at regular intervals, adding protective layers between the skin and the medical device where possible, using a foam securement device to provide padding and prevent friction, and carefully monitoring the moisture associated with the device may decrease the incidence or severity of MDRPIs in the hospitalized patient. Surprisingly, a study reviewing hospitalized patient data collected through state-mandated reporting in Minnesota noted that 63% of reported MDRPIs had no documentation of device removal at regular intervals for pressure relief, an inspection of the skin, or cleansing of the area; 74% of those same MDRPIs were at Stage 3 or higher on discovery (Delmore & Ayello, 2017; Jackson et al., 2019).
Children and neonates are a population that is also at increased risk for medical device-related HAPIs. Skin immaturity has been identified as a significant pressure injury risk factor in neonates. For neonates under 30 weeks gestation, the stratum corneum is not fully developed, and for neonates over 30 weeks gestation, the stratum corneum is only 2-3 cells thick. This skin is highly fragile and provides an inadequate barrier, and is therefore highly susceptible to breakdown. Children and neonates are also at higher risk for HAPIs due to their size and weight (NPIAP, 2019).
Current skin assessment tools may not identify the risk from medical devices as their focus is on risk factors such as nutritional status, age, or illness. Additionally, patients may be at risk for an MDRPI even where these factors are not present. Injuries from medical devices can occur in any patient without proper assessment, prevention, or early intervention. The development of new tools to identify risk or actual injury from medical devices may be needed, considering the limitations of current skin assessment tools. A robust exploration into quality improvement (QI) initiatives should be considered by healthcare organizations that include higher levels of vigilance in assessment, product selection, and efficient reporting strategies. QI initiatives should focus on a more explicit recognition of population or situational risk associated with medical devices (Jackson et al., 2019).
In 2016 the NPIAP also included mucosal membrane pressure injuries. These pressure injuries are found on mucosal membranes following medical device use. Staging is not possible with these pressure injuries due to the location and anatomy of the tissue. Mucosal membrane pressure injuries are found in the gastrointestinal (GI) tract, nasal passages, urinary tract, and tracheal lining (NPIAP, n.d.).
Prone Positioning
During the COVID-19 pandemic, many patients presented with severe respiratory distress and low partial oxygen pressure (PaO2). As the treatment for COVID-19 evolved, interventions typically used in patients with acute respiratory distress syndrome (ARDS) were implemented. One such intervention was to place the patient in a prone position. This positioning increases oxygenation and decreases mortality in patients with ARDS. To reduce mortality rates of patients with ARDS, the patient must be placed in a prone position for over 12 out of 24 hours. This positioning increases the incidence of pressure injuries on the face, cheekbones, thorax, and anterior bony prominences (Johnson et al., 2021).
Skin Assessment
To properly determine HAPI risk, a thorough head-to-toe skin assessment must be completed by the healthcare professional (HCP). Elements of a comprehensive skin assessment include skin temperature, color, moisture, turgor, and integrity. To properly assess skin temperature, the HCP should use the dorsal side of the hand instead of the palmar side to touch the skin and determine if the skin is warm or cool. It is essential to assess symmetrical body areas bilaterally to compare if temperature changes are unilateral or bilateral. While assessing the skin for temperature changes, the HCP should also evaluate the same areas for dryness or moisture. Macerated skin from excessive moisture may feel soft or boggy. Determine if the moisture or dryness is localized to one location or if it is generalized. The HCP must assess the skin under adequate lighting to determine skin color changes. If needed, a penlight can illuminate hard-to-see areas such as the sacrum. It is essential to know the patient's baseline skin tone to determine if changes have occurred; for symmetrical body parts, assess the area bilaterally to determine if color changes are unilateral. For any areas with color change, depress the site to determine if the discoloration is blanchable or non-blanchable. Assessing skin turgor includes briefly pinching the skin near the clavicle or back of the hand and releasing the skin. A typical finding consists of the skin returning in 0-1 seconds. When the skin remains upright, it is known as tenting, which is an abnormal finding indicative of dehydration or connective tissue disease. An older person's skin may take up to 20 seconds to return to normal without the presence of dehydration due to skin elasticity changes. Skin integrity is vital to a thorough skin assessment. The HCP should assess the entire body for the loss of integrity, such as cracks, openings, excoriations, or lesions. A comprehensive skin assessment is critical for the proper risk assessment of an individual (Agency for Healthcare Research and Quality [AHRQ], 2014).
Pre-existing pressure injuries, or any alterations in skin condition, indicate a higher risk for the development of subsequent injuries. If the patient's acuity and the length of hospital stay increase, the opportunity for injury to the skin also rises. Maintaining good nutritional status, managing medical needs, and increasing mobility are all actions that reduce the risk of injury. Identifying risk allows for early intervention, which may improve outcomes. Once an injury has occurred, staging skin injuries is essential to direct the most appropriate management based on evidence and current guidelines (NPIAP, 2019).
Risk Assessment Tools
The elements of a comprehensive skin tool include skin temperature, color, moisture, turgor, integrity, and patient mobility. Many tools are available to the healthcare team, yet the most common include the Braden and Norton Scales. Both scales have high levels of validity and reliability in identifying high-risk patients. The HCP should use a skin assessment tool to measure the risk of skin injury as soon as possible after admission and repeat per policy (AHRQ, 2017).
Braden Scale
The Braden Scale has been in use since 1988. It is the most commonly used tool for predicting pressure injuries and skin breakdown in hospitals and long-term care facilities (The Joint Commission, 2022b). The Braden Scale estimates the risk for pressure injuries by assessing the following (AHRQ, 2014; Bergstrom et al., 1987):
Sensory perception: the patient's ability to respond to pressure-related pain or discomfort should be assessed as completely limited, very limited, slightly limited, or no impairment present. Completely limited indicates that the patient is unresponsive to painful stimuli due to either sedation or a decreased level of consciousness (LOC) or has a limited ability to feel pain. Very limited indicates that the patient is only responsive to painful stimuli, characterized by moaning or increased restlessness, or has a decreased ability to feel pain over half of their body. Slightly limited indicates that the patient can respond to verbal commands but cannot communicate feeling discomfort or the need to change positions or has sensory impairment in one or two extremities. No impairment indicates that the patient can respond to verbal commands and has no sensory deficit impairing the ability to feel pain or discomfort.
Moisture: the degree to which the patient's skin is exposed to moisture and whether the skin is constantly moist, often moist, occasionally moist, or rarely moist should be established. Constantly moist indicates that dampness is detected every time the patient is assessed, moved, or turned. Very moist indicates that the skin is often but not constantly moist, requiring a linen change more than once per shift. Occasionally moist indicates that the skin is moist sometimes and requires an extra linen change at least once daily due to moisture. Rarely moist suggests that the skin is dry, and linens only need to be changed routinely.
Activity: whether the patient is bedfast, chairfast, walks occasionally, or walks frequently should be evaluated. Bedfast indicates that the patient is confined to the bed. Chairfast suggests that the patient's ability to bear weight is limited, and assistance is needed to transfer from the bed to a chair. Walks occasionally indicates that the patient can ambulate short distances with or without assistance, but most of the time is spent in a chair or bed. A score of walks frequently indicates that the patient ambulates outside of their room at least twice daily and in their room every two hours.
Mobility: the patient's ability to move when changing body position and whether they are completely immobile, have very limited mobility, have slightly limited mobility, or have no mobility limitations is measured. Completely immobile indicates that the patient cannot make slight position changes without assistance. Very limited indicates that the patient can make occasional or minor position changes of their body or extremities but cannot make significant position changes without assistance. Slightly limited indicates that the patient can make frequent but slight changes to body and extremity position. No limitations indicate that the patient can position themselves without assistance.
Nutrition: the patient's food intake (including parenteral and enteral nutrition) is assessed as very poor, probably adequate, adequate, or excellent. A patient who rarely eats more than one-third of a meal, is NPO, or has been restricted to clear liquids or parenteral therapy for more than five days is considered to have very poor nutrition. A patient that eats only half of the food offered or receives less than optimal amounts of liquid diet or enteral nutrition is considered to have a nutritional status of probably inadequate. A patient who eats over half of most meals or receives enteral feeding at optimal levels is considered to have an adequate nutrition assessment. Excellent nutrition indicates that the patient consumes most of every meal offered, occasionally eats between meals, and does not require supplementation.
Friction and shear: this measures the patient's ability to move in the bed or chair and determines whether their risk of experiencing friction and shear is a problem, potential problem, or no apparent problem. A patient who requires maximum assistance in repositioning, frequently slides down in the bed or chair, or has spasticity or contractures has a problem with friction and shear. A patient with a potential problem requires minimal repositioning assistance, occasionally slides down in a chair or bed, and slides against the sheets during a move. A patient with no apparent problem can move in the bed or chair independently, have the muscle strength to lift themselves during a move, and maintain proper positioning in a chair or bed.
Each category is given a score of 1-4 (except friction and shear, which is scored 1-3; see Table 3 below). These are then added to determine the individual's risk for skin-related issues during admission. Total scores may range from 6 to 23. The higher the score, the lower the risk for pressure injuries. A score of 18 or less indicates an at-risk status for developing a pressure injury (see Table 4 below). HCPs should keep in mind that patients could potentially have a low-risk total score yet have an increased risk in a single category; thus, a review of the information may give opportunities to avoid injury and should be considered when developing a care plan. After determining the risk, interventions are instituted accordingly to decrease the risk and prevent the development of skin breakdown (Bergstrom et al., 1987; Hovan, 2021; NPIAP, 2019).


Norton Scale
The Norton scale was created in 1962 in England. It was the first-ever pressure injury risk assessment tool designed. It is mainly used for elderly patients in long-term care settings. The scale is easy to use and effectively recognizes the risk of pressure injuries or other skin concerns. The Norton scale has five categories: physical, mental, activity, mobility, and incontinence. Within each category, the patient is given a score of 1-4 based on characteristics defined by the scale (see Table 5 below). The score for each of the five categories are added together with a sum between 5 and 20 (see Table 6 below). A score of 14 or less indicates the patient is at risk of developing a pressure injury. Like the Braden score, the lower the Norton score, the higher the risk (AHRQ, 2014; Spinal Cord Injury Research Evidence [SCIRE], n.d.).

The Braden Scale is considered more precise than the Norton Scale due to the broader range of clinical factors; therefore, it is more widely used. When using a risk assessment scale, it is essential to include a comprehensive risk assessment of modifiable and non-modifiable risk factors not included in the risk assessment, including those outlined previously in the section on general and medical device risk factors (NPIAP, 2019; SCIRE, n.d.).
The NPIAP (2019) recommends that a full skin assessment using a validated assessment tool such as the Braden Scale or Norton Scale is completed as soon as possible but no more than eight hours after admission. In contrast, the National Database of Nursing Quality Indicators (NDNQI, 2018) recommends that the skin assessment be completed within 24 hours of admission to identify any pre-existing injuries and assess the risk for future injury. The nurse should also remember that risk can exist without a high score on the skin assessment tool. Any change in condition or acuity that could increase the risk requires a repeat assessment. Along with each risk assessment, a comprehensive skin assessment with documentation should be completed and maintained in the medical record. While there is no universally accepted risk assessment, each facility should have a structured risk assessment that is consistently applied. Each institution should also have a risk-based prevention plan for patients identified at risk for developing pressure injuries. The physical assessment and skin risk assessment tool results determine the risk for pressure injury (NPIAP, 2019).
Prevention
Severe pressure injuries are considered "never events," critical medical errors that should never happen. CMS classifies HAPIs as preventable and no longer reimburses hospital systems treating/managing them (AHRQ, 2019; Miller et al., 2019).
Various interventions have been discussed in the literature to reduce the number of HAPIs in today's clinical setting, including intervention bundles. A bundled intervention is a "structured way of improving the processes of care and patient outcomes; a small, straightforward set of evidence-based practices-generally three to five-that, when performed collectively and reliably, have been proven to improve patient outcomes" (Institute for Healthcare Improvement [IHI], n.d., para. 1). An example of a bundled intervention developed for patients at risk for pressure injuries is called the SKIN bundle. After recognizing the threat, the nurse or healthcare team implements treatment such as the SKIN bundle (IHI, n.d.). The acronym "SKIN" stands for
surface selection
keep turning patients
incontinence management
nutrition (IHI, n.d.)
By applying the SKIN bundle, the bedside nurse is the first line of defense in pressure injury prevention. Interventions such as the SKIN bundle focus the interdisciplinary team on caring for the patient to decrease the risk and prevent injuries. It is essential to understand how the different components are related by following a clinical pathway to implement a bundle successfully. Clinical pathways provide a guide for each step. Benefits of clinical pathways include enhanced standardization of care between healthcare facilities, provision of evidence-based care, improved patient outcomes, improved care planning, and enhanced interdisciplinary collaboration (AHRQ, 2014; IHI, n.d.).
Regardless of the acronym, aspects of an intervention bundle, or policies and procedures of the facility, those responsible for patient care should work to utilize the tools available for assessment and prevention. HCPs should be familiar with the latest guidelines for pressure injury prevention and implement evidence-based care for their patients. A multi-pronged approach to pressure injury prevention is the best practice. Organizations typically adopt multiple strategies to decrease the risk of HAPIs. The IHI (n.d.) further identifies six key steps that assist healthcare facilities in meeting their goals to prevent pressure injuries.
Conduct a pressure injury assessment for all patients, utilizing the Braden or Norton risk assessment tools.
Reassess pressure injury risk for all patients at least daily.
Inspect the skin of at-risk patients daily.
Manage moisture from diaphoresis or incontinence.
Optimize nutrition and hydration and provide supplementation if needed.
Minimize pressure by offloading pressure areas and changing patient positioning frequently.
Organizations must determine the best methods based on the guidelines and the patient population they serve. Budget, workforce, and resources, in addition to national guidelines, drive the policies and procedures for patient care (NPIAP, 2019).
MDRPI Prevention
The NPIAP guidelines recommend that medical devices be selected and adjusted individually to exert the least amount of pressure or shearing forces. For instance, HCPs should use the softest device or securement products that promote the slightest friction or shearing force for any tubing, such as an endotracheal tube, urinary catheter, or tracheostomy tube. Medical devices such as helmets, halo vests, or restrictive devices should fit correctly to avoid excessive pressure. All devices should be applied according to the manufacturer's specifications to prevent unintended injury and liability to the facility. The focus should be on securing any medical device appropriately and using padding or cushioning against the tissue (NPIAP, 2019). Recommendations for the assessment of skin surrounding or beneath a medical device and prevention of MDRPIs include (NPIAP, 2019):
• Increase the frequency of skin assessments and observe for increased edema or irritation.
• Educate the patient and family on risks related to the medical device, including recognizing and reporting injuries or concerns.
• If an injury occurs, classify the MDRPI using the International NPIAP Pressure Classification system (see Table 1).
• Remove devices as quickly as appropriate for the medical condition.
• Maintain proper skincare under and around the medical device, keeping the area clean and dry.
• Reposition the patient regularly to decrease pressure from the medical device.
• Reposition or rotate the position of the medical device regularly, when possible, to avoid ongoing pressure on the same area.
• Provide cushioning or supportive devices to decrease pressure on the underlying tissue.
• Prophylactic dressings for pressure, such as a soft foam silicone dressing, may reduce the risk of skin breakdown. The NPIAP guidelines have further information on the ideal characteristics of prophylactic dressings, including the ability to assess skin under the dressing, ease of removal and reapplication, location of the device on the patient's body, or ability to manage body fluids around the dressing.
National Patient Safety Goals
The Joint Commission endorses the National Patient Safety Goals (NPSGs), which are standards addressing the highest priority patient safety issues in all healthcare settings. NPSG #14 is to prevent HAPIs. This goal notes that each patient's risk should be identified, and action should be taken to address any pressure injuries discovered during the skin assessment. The goal states that most pressure injuries can be avoided through preventative measures, and damage can be decreased if injuries are identified early, preferably at Stage I. The healthcare organization is expected to have a written plan to identify risk and prevent pressure injuries; perform an initial skin assessment that identifies risk for pressure injuries; use a skin risk assessment tool such as the Braden or Norton scales to validate risk assessment; reassess patient skin at specified intervals as determined by the organizational policies; and take actions appropriate for the risks identified during the evaluation that prevents injury to the patient and protects them from external mechanical forces. Also, there should be education for staff that identifies risk factors for pressure injuries and prevention techniques as defined by the organization based on the latest evidence and guidelines (AHRQ, 2017; The Joint Commission, 2022a).
Management of Pressure Injuries
The NPIAP (2019) Clinical Practice Guideline of Interventions for treating pressure injuries examines wound bed preparation. This is a clinical concept, which is a holistic, systematic approach to evaluating and treating wounds that allow a natural progression toward wound healing. The goal of wound bed preparation is "to promote a well-vascularized wound bed, free from nonviable tissue and excess exudate, and with a reduced bacterial burden and reduced edema, that is optimal for the development of healthy granulation tissue" (NPIAP, 2019, p. 235). The acronym TIMERS, describing the components of wound bed preparation, is defined as follows:
tissue management
- infection and inflammation control
- moisture balance
- epithelial edge advancement
repair and regeneration
social factors (NPIAP, 2019)
Routine assessment and wound care driven by TIMERS will remove the barriers that delay routine healing in chronic wounds. Debridement of necrotic tissue and the associated bacterial and cellular burden stimulate healthy tissue growth. Wound cleansing removes remnants of old dressings and decreases the number of bacteria in the wound bed. If there are other particles or devitalized tissue, debridement is needed. Cleansing should be gentle to avoid damaging new tissue growth. Aseptic technique with sterile products should be utilized for immunocompromised patients or if the wound enters a sterile body cavity. Normal saline is recommended for wound cleansing for clean pressure injuries or those without any signs of infection. Antimicrobial cleansing solutions should be used for wounds with confirmed or suspected infection. Wounds with sinus tracts or tunneling should be cleansed with caution as some of the solution could be retained in the wound, causing further injury. The wound cleansing should include sufficient pressure to adequately cleanse the wound but avoid damaging tissue or driving bacteria further into the wound. All cleansing solutions should be single-patient use and disposed of properly to prevent cross-contamination. The surrounding skin should also be cleansed, taking particular care for wounds on the coccyx or perineal areas (NPIAP, 2019).
Debridement
When debridement is needed, many factors should be considered. The procedure can be excruciating, and pain management should be part of the care plan. Devitalized tissue that is thick or leathery and discolored, including yellow, green, tan, grey, brown, or black, should be debrided to promote healing. Bacteria grows in necrotic tissue and further delays wound healing. However, the patient's overall condition and ability to tolerate the debridement is included in this decision. Indications for debridement may consist of biofilm (collection of one or more types of organisms that form a slimy build-up), delayed wound healing, or failure to respond to standard wound care (NPIAP, 2019). Debridement of pressure injuries may utilize the following techniques:
Surgical debridement is performed by a specialty or primary HCP. Surgical debridement removes necrotic tissue, cellular debris, wound exudate, or eschar from the wound bed to facilitate healing. This invasive procedure uses sharp and sterile instruments to excise the nonviable materials from the wound bed. For wounds requiring this intervention, the interdisciplinary team must support the procedure and perform subsequent wound care and assessments (Pilgrim & Heering, 2017).
Mechanical debridement has been completed for all wound types using wet-to-dry dressings over the last few decades. With this type of mechanical debridement, the wound is cleansed, and a moist dressing is applied to the wound bed. After the dressing has dried, it is removed. The goal is to pull away the top layer of tissue within the wound with the dried dressing. This removes exudate, necrotic or infected material, and foreign bodies. The disadvantage of a wet-to-dry dressing is that it is non-selective; the entire top layer of the wound is removed without discerning between viable and nonviable tissue. This type of debridement can be excruciating for the patient, so pre-medication with analgesics is indicated to increase patient comfort. Patients on anticoagulant medications or with underlying coagulopathy may have significant bleeding with mechanical debridement, so these individuals require extra care. Although mechanical debridement with wet-to-dry dressings is cost-effective, dressing changes must be completed frequently, increasing overall supply cost. New forms of mechanical debridement include hydrotherapy, pulsative lavage, and ultrasonic mist debridement (Avital & Schub, 2018).
- Hydrotherapy (also known as hydrosurgery or whirlpool) combines lavage and sharp debridement instrumentation. In comparison to moist dressings, hydrotherapy debridement is well tolerated by patients with arterial and venous wounds. It is faster and more cost-effective than traditional debridement methods.
- Pulsatile lavage combines intermittent lavage with suction to loosen and remove nonviable tissue from the wound bed. Although this is fast and effective, caution must be taken not to damage underlying structures such as blood vessels, bones, and tendons. Pulsatile lavage is also costly since the equipment is single-use only.
- Ultrasonic mist debridement uses acoustic energy to remove nonviable tissue from the wound bed. When used in conjunction with standard wound care, ultrasonic mist debridement can safely and effectively remove necrotic tissue and promote wound healing.
- Biologic debridement, otherwise known as maggot debridement therapy, uses sterile, medical-grade larvae of the Lucilia sericata species of the green bottle fly to remove necrotic tissue from the wound bed. It is beneficial in large wounds needing painless removal of necrotic tissue. Proteolytic enzymes are released from the larvae to dissolve necrotic tissue. The wound bed is cleaned, and sterile larvae are applied to the wound bed and then covered with a mesh-like, air-permeable dressing for 1-3 days, after which the dressing and larvae are removed. If further debridement is needed, the process can be repeated. Wounds should never be allowed to close over the larvae, and they should not be left in the wound bed if they die, as this increases the risk of allergic reaction or infection. Larvae used for this treatment are considered contaminated and should be disposed of properly by sealing them in a plastic bag and placing it in a biohazard container for incineration (Manna et al., 2021; Schub & Walsh, 2018; Wernick et al., 2021).
Enzymatic or chemical debridement dissolves necrotic tissue, cellular debris, wound exudate, and foreign materials using commercial enzyme products. One commonly used medication in this category in the US is collagenase SANTYL ointment. The active ingredient is from the bacterium Clostridium histolyticum, which breaks down collagen in necrotic tissue. Patients receiving this treatment are at an increased risk for systemic infection related to blood contamination with bacteria from the wound bed. Silver and iodine can inactivate collagenase, so dressings with these ingredients should be avoided after applying the collagenase ointment (Caple, 2019).
Autolytic debridement uses the body's enzymes and healing processes to rehydrate, soften and liquefy, then expel the necrotic tissue from the wound. Occlusive dressings are often used to keep the body's fluids in the wound bed and maintain a moist healing environment. Dressings used for autolytic debridement include foam dressings, hydrogel sheets, honey dressings, hydrocolloid dressings, and amorphous hydrogel. These should not be used in infected wounds, those that need to be urgently debrided for best outcomes, or wounds with large amounts of necrotic tissue, undermining, or tunneling. Immunocompromised patients should not undergo autolytic debridement (Caple & DeVesty, 2019).
Bacteria are present on all skin surfaces, and when the skin integrity is breached, bacteria present on the surface can enter the wound. When the bacterial presence increases and wound damage occurs, an infection is present. Healthy individuals can usually avoid developing an infection due to their immune system defense response, yet an immunocompromised patient will have a decreased ability to fight the bacteria. "The number of bacteria and their effect on the patient are categorized as: contamination, colonization, local infection, spreading infection, and systematic infection" (NPIAP, 2019, p. 251). Microorganisms may multiply, invade, or damage tissues in or around the wound bed, delay healing, and cause systemic responses. Infection is present if a pressure injury is not healing due to the bacteria in the wound bed. Biofilms may be the source of wound infection or delay healing. The biofilms must be removed by debridement and prevented from reforming by using antiseptics and antimicrobial dressings (NPIAP, 2019). Other signs or symptoms of infection are:
- erythema that extends past the wound edges
- induration of the tissue
- increasing or change in pain
change in temperature
- purulent drainage
- increasing wound size
- systemic reactions including fever, malaise, lymph node enlargement, confusion, or anorexia (particularly in the older adult; NPIAP, 2019)
To properly manage wound infection, wound cultures may be required to determine the appropriate treatment based on the organism involved. If a biofilm is recognized, a tissue biopsy may be necessary. Other healthcare team members should be notified of signs and symptoms of infection, including dieticians, nurses, and providers, such as vascular and wound care specialists. Poor nutritional status, lack of glycemic control, certain medications, and inadequate circulation are possible causes of an infection. Any deficits in these areas should be further explored and managed by the healthcare team (NPIAP, 2019).
Treatment of infected wounds can include systemic antibiotics, topical antiseptics, silver Silvadene, medical-grade honey, or topical antibiotics. (NPIAP, 2019). Wound dressings should be selected based on the following:
- ability to keep the wound bed moist
- need to address the bacterial burden
- type and amount of wound exudate
- condition of the tissue in the wound bed
- status of the surrounding skin
- injury stage and location
- presence of tunneling or undermining
- goals of the patient and the healthcare team (NPIAP, 2019)
Antibiotic therapy for treating a wound infection commonly includes intravenous (IV) and oral antibiotics to elicit systemic effects. Topical antibiotic use should be limited except when the benefits outweigh the risk of side effects and bacterial resistance. The most common oral antibiotics prescribed for wound infections include amoxicillin-clavulanate (Augmentin), cephalexin (Keflex), clindamycin (Cleocin), doxycycline (Vibramycin), or trimethoprim-sulfamethoxazole (Bactrim). Common IV antibiotics used to treat wound infections include erythromycin (Erythrocin), cefazolin (Ancef), cefoxitin (Mefoxin), and cefotetan (Cefotan). Specific side effects of antibiotics are greatly dependent on their administration route and classification. General side effects of IV antibiotics include swelling, redness, and pain at the injection site. Common side effects of oral antibiotics include diarrhea, nausea, bloating, and abdominal pain (Nelson, 2021; NPIAP, 2019; Singhal, 2021).
Dressings
The proper dressing for a wound will support healing at a faster rate. Dressing types will likely change throughout the healing stages, and the nurse will need to assess the injury and update the dressing throughout the trajectory of care. Unfortunately, the cost is essential to consider in determining wound care products. Comfort and usability are also important factors, as the patient or family members may be performing the wound care once the patient is discharged from the health care facility. Staff workload and patient compliance should be considered when determining the frequency of dressing changes. Newer treatment modalities require less frequent changes and can stay in place for longer with optimal results (NPIAP, 2019).
Hydrocolloid dressings are moisture-retentive dressings used to protect wounds with a small to moderate amount of drainage. These are often used to treat non-infected Stage I through Stage IV pressure injuries, partial to full-thickness wounds, abrasions, and necrotic wounds. Hydrocolloids can function as a secondary dressing with alginates or wound fillers that need to remain in the wound bed for an extended time. Do not use hydrocolloids with excessive exudate in wounds. Do not cover enzymatic debriding agents, gels, or ointments with hydrocolloid dressings. Examples of hydrocolloid dressings are DuoDerm or Nu-Derm (NPIAP, 2019; Smith & Caple, 2019).
Hydrogel dressings contain a high water/glycerin content within a gel base and are used to provide moisture to the wound bed. The moist environment facilitates the debridement of necrotic tissue and tissue granulation. The amorphous hydrogel can be applied in a layer over the wound surface, or a hydrogel impregnated gauze can be used to fill dead spaces in deep wounds such as Stage III or IV pressure injuries. These dressings should not be used with moderate to heavy wound exudate or when the goal of care is to maintain dry eschar. Use amorphous hydrogel dressings on injuries that are not infected but are granulating. Gravity-dependent body areas such as the lower legs benefit from amorphous hydrogel dressings. Hydrogel sheets can treat dry bed wounds and are often used on non-moving or nondependent body surfaces. Hydrogel dressings can contain allergens such as iodine, silver, or sodium carboxymethyl cellulose and should not be used in patients with known sensitivities or allergies to these products. Examples of hydrogel dressings are Aquasite gel/sheets or Derma-gel (Caple & Walsh, 2018; NPIAP, 2019).
Alginate dressings are used for highly exudative wounds and contain alginic acid from seaweed covered in calcium/sodium salts. These dressings are highly absorbent, absorbing up to 20 times their weight in exudate. The alginate dressing should be irrigated first to aid in removal and then gently removed. Alginate dressings may also contain controlled-release ionic silver. These dressings interact with the serum to form a hydrophilic gel in the wound bed; they are utilized concurrently with infection treatment. These dressings have minimal antimicrobial properties and should not be used as a primary treatment for infected wounds. Examples of alginate dressings are Maxsorb or Megisorb (NPIAP, 2019; Walsh & Schub, 2018).
Foam dressings can be constructed from either foam that draws in fluid and physically expands as it retains the drainage or pseudo-foam that contains absorbent materials such as viscose and acrylate fibers designed to hold extra fluid. These are best for wounds with moderate to heavy drainage. They can be used as a primary or secondary dressing on wounds and remain in place for up to seven days. Most are non-adhesive and can easily be used on those with allergies to adhesives. Antimicrobial foam dressings can be used on infected wounds. Choose foam dressings for heavy drainage from Stage II or III pressure injuries. Examples of foam dressings are Aquacell Foam or Optifoam (Mennella & Schub, 2017).
Gauze and non-woven dressings have been used for wound care for decades, but with the advancement of new materials designed to accelerate healing, these materials are rarely used in modern-day wound care. Daily dressing changes are required with these materials to manage drainage effectively. Gauze dressings can cause further tissue damage in open pressure injuries, particularly if they are removed dry. The 2019 NPIAP guideline recommend avoiding wet-to-dry dressings in pressure injuries. It is acceptable to use gauze dressings when other moisture-retentive dressings are not available; however, wound bed moisture must be maintained. Further, the gauze dressing can be used as a cover or loose packing for deep pressure wounds. Only use saline-moistened gauze when other forms of moisture-retentive dressings are not available. Multiple layers of gauze should not be used to control drainage as that can serve as a source of infection. Several studies have shown that other dressings have higher success rates with wound healing, and gauze dressings can promote infection or delay wound healing (NPIAP, 2019).
Bioactive dressings improve wound healing and are derived from natural sources, proteins, or tissues. These products are especially useful in Stage II and III pressure injuries. Examples are collagen dressings and medical-grade honey (Wood, 2021).
Use silver-impregnated dressings in clinically infected wounds heavily colonized with bacteria (NPIAP, 2019).
Use cadexomer iodine dressings for excessive wound drainage. However, these should be used with extreme caution and avoided in individuals with renal failure, thyroid disorders, or known iodine sensitivity. Breastfeeding or pregnant women should not use cadexomer iodine dressings since the risk of systemic absorption is high (NPIAP, 2019).
Silicone dressings are used as a wound contact layer to promote atraumatic dressing changes or prevent periwound injury around fragile tissue. They will not chemically interact with the wound and are easy to remove (NPIAP, 2019).
Incorporate collagen matrix dressings to treat Stage III and IV pressure injuries. The application of collagen has been shown to promote wound healing in at least one study, but the cost of the product is high (NPIAP, 2019).
Hyperbaric Oxygen Therapy
Hyperbaric oxygen therapy (HBOT) may be used on chronic wounds to promote wound healing. Injuries that are not healing are typically hypoxic, and increasing oxygen tension and pressure by various methods can stimulate healing. HBOT promotes muscle and nerve regeneration by stimulating angiogenesis or developing new blood vessels. The treatments can be done on limbs placed in a limb-encasing device or a full-body chamber. HBOT has been in use for over 40 years and should be part of an interdisciplinary team approach with a comprehensive plan of care for wound healing that includes strategies for extensive vessel disease, glycemic abnormalities, nutritional deficiencies, infection, and the presence of necrotic tissue. Contraindications for systemic HBOT are asthma, claustrophobia, COPD, eustachian tube dysfunction, pacemaker, high fever, epidural pain pump, pregnancy, seizures, and upper respiratory infections. Absolute contraindications would include a pneumothorax, severe respiratory disease, and recent use of specific medications, such as chemotherapy, disulfiram (Antabuse), or mafenide (Sulfamylon; Kaur et al., 2019; Mechem & Manaker, 2020; Wernick et al., 2021).
Negative Pressure Wound Therapy
Negative pressure wound therapy (NPWT), also called vacuum-assisted closure, applies suction or negative pressure to the wound bed. This therapy promotes wound healing by removing excess drainage, stimulating vascularization, and supporting the closure of wound edges or margins. Negative pressure creates mechanical stress that promotes growth factor expressions, angiogenesis, and granulation tissue growth. The negative pressure opens the capillary beds and draws blood to the wound area, reduces edema and bacterial colonization, and provides a moist wound bed that promotes healing. This treatment is often used on deep or full-thickness Stage III or IV pressure injuries. Pain is commonly reported as an adverse reaction and should be proactively managed during treatment. This treatment should not be used in individuals at increased risk of bleeding as life-threatening hemorrhage could result (Gestring, 2022; Kaur et al., 2019; Wernick et al., 2021).
Pain Control
Pain is an often-overlooked aspect of pressure injuries and wound care. Although initial pain can indicate an issue with the skin, it can become chronic and debilitating. Many patients report that the pain experienced during wound care is as painful as the initial injury. Pain can increase patient fear, anxiety, and depression, negatively impacting wound healing. A patient with a wound may experience different types of pain. The injury itself may cause neuropathic pain, wound treatments may cause nociceptive pain, and anticipatory pain can be a factor for patients undergoing painful wound treatments. Factors that increase pain are the depth of the wound, structures involved, infection, and other concurrent injuries or conditions. The nurse should complete a pain assessment to determine all aspects of the pain, including location, duration, exacerbating and relieving factors, quality, and severity, using a patient-appropriate pain scale. It is essential to pre-medicate the patient with analgesics before debridement or other wound care that may stimulate pain. The HCP must time medication administration according to the expected onset of action and duration to ensure coverage during dressing changes or debridement (Jones & Williams, 2017). There are also non-pharmacologic interventions that the HCP can use to reduce pain and increase patient comfort during wound care activities.
Distractions can help decrease pain, including watching television, playing games, or reading a book;
The HCP should space out care to give the patient uninterrupted rest time in a quiet environment;
Reduce anxiety levels with music therapy or other guided imagery techniques;
Position the patient for comfort during any procedures or dressing changes;
When possible, limit the number of dressing changes by using dressings that can remain in place for more extended periods;
Utilize dressing types, tapes, and adhesives that do not adhere to the wound bed or pull at the wound;
Allow the patient to choose times for treatments or dressing changes to create a feeling of independence or control and decrease anxiety;
Consider alternative therapies such as hypnosis to reduce pain (Chester et al., 2016).
Future Opportunities
Future opportunities to promote healing in pressure injuries include but are not limited to biological dressings comprised of animal materials, human skin cells, plant materials, synthetic materials, or a mixture of these. Examples are skin substitutes, xenografts, allografts, or collagen dressings. Currently, there is insufficient evidence to support their use (NPIAP, 2019).
One treatment that is gaining popularity for various ailments is platelet-rich plasma (PRP). To make PRP, blood is drawn from the patient and centrifuged to create the PRP. The PRP is then administered by injection to the injured area. PRP may present opportunities for escalated wound healing. Current investigations for the recovery of pressure injuries include recombinant platelet-derived growth factor, basic fibroblast growth factor, granulocyte-macrophage colony-stimulating factor, or bone marrow nuclear cells. Stage III and IV pressure injuries with delayed wound healing may benefit from a recombinant platelet-derived growth factor. These treatments are in the early stages of use, not first-line treatments. Nevertheless, these treatments demonstrate opportunities for improvement or complete healing for persistent chronic wounds (Dreher, 2022; NPIAP, 2019).
Summary
Pressure injuries are costly to both the organization and the patient. Litigation is at an all-time high for pressure injuries, and care for these patients is not reimbursable. Education for all HCPs is needed to ensure that all interdisciplinary team members are aware of the risks, appropriate interventions, and the overall cost to the organization of a HAPI. It is easy to provide evidence to support even costly preventative interventions compared to the cost of even one pressure injury. Nurses must be advocates that promote appropriate staffing, preventative devices, and other tools needed to deliver safe and effective care to decrease the risk of pressure injuries (IHI, n.d.; NPIAP, 2019).
References
Agency for Healthcare Research and Quality. (2014). Preventing pressure ulcers in hospitals. https://www.ahrq.gov/patient-safety/settings/hospital/resource/pressureulcer/tool/pu7b.html
Agency for Healthcare Research and Quality. (2017). Pressure injury prevention in hospitals training program. https://www.ahrq.gov/professionals/systems/hospital/pressureinjurypxtraining/index.html
Agency for Healthcare Research and Quality. (2019). Never events. https://psnet.ahrq.gov/primer/never-events
Avital, O., & Schub, T. (2018). Wound care: Performing mechanical debridement. CINAHL Nursing Guide. Retrieved April 19, 2022, from https://research.ebscomedical.com/eds/detail?db=nup&an=T706154
Babagolzadeh. (2012). Wound stage [Image]. https://commons.wikimedia.org/wiki/File:Wound_stage.jpg
Bergstrom, N., Braden, B. J., Laguzza, A., & Holman, V. (1987). The Braden Scale for predicting pressure sore risk. Nursing Research, 36(4), 205-210. https://pubmed.ncbi.nlm.nih.gov/3299278/
Betts, G., Desaix, P., & Johnson, E. (2013). Structure of the skin [Image]. https://commons.wikimedia.org/wiki/File:501_Structure_of_the_skin.jpg
Black, J., & Maegley, J. (2019). Help-U to prevent HAPI: A change project to attain zero HAPIs. MEDSURG Nursing, 28(1), 31-47. https://www.thefreelibrary.com/Help-U%20to%20Prevent%20HAPI:%20A%20Change%20Project%20to%20Attain%20Zero%20HAPIs.-a0577027471
California Hospital Patient Safety Organization. (2017). By the numbers: CHPSO pressure injury data. https://www.chpso.org/post/numbers-chpso-pressure-injury-data
Camacho-Del Rio, G. (2018). Evidence-based practice: Medical device-related pressure injury prevention. https://www.myamericannurse.com/medical-device-pressure-injury-prevent/
Caple, C. (2019). Wound care: Performing chemical debridement. CINAHL Nursing Guide. Retrieved April 19, 2022, from https://research.ebscomedical.com/eds/detail?db=nup&an=T706160
Caple, C., & DeVesty, G. (2019). Wound care: Performing autolytic debridement. CINAHL Nursing Guide. Retrieved April 19, 2022, from https://research.ebscomedical.com/eds/detail?db=nup&an=T703954
Caple, C., & Walsh, K. (2018). Wound dressings: Hydrogel - applying. CINAHL Nursing Guide. Retrieved April 19, 2022, from https://research.ebscomedical.com/eds/detail?db=nup&an=T704148
Centers for Medicare and Medicaid Services. (2021). Hospital-acquired conditions. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalAcqCond/Hospital-Acquired_Conditions
Chester, S. J., Stockton, K., De Young, A., Kipping, B., Tyack, Z., Griffin, B., Chester, R. L., & Kimble, R. M. (2016). Effectiveness of medical hypnosis for pain reduction and faster wound healing in pediatric acute burn injury: study protocol for a randomized controlled trial. Trials, 17, 223. https://doi.org/10.1186/s13063-016-1346-9
Delmore, B.-A., & Ayello, E. A. (2017). Pressure injuries caused by medical devices and other objects: A clinical update: A review of practical resources, including mnemonics, to aid in prevention and identification. American Journal of Nursing, 117(12), 36-47. https://doi.org/10.1097/01.NAJ.0000527460.93222.31
Dreher, G. (2022). Platelet-rich plasma (PRP) injections. https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/plateletrich-plasma-prp-treatment
Gestring, M. (2022). Negative pressure wound therapy. UpToDate. Retrieved April 10, 2022, from https://www.uptodate.com/contents/negative-pressure-wound-therapy
Hovan, H. (2021). Understanding the Braden Scale: Focus on sensory perception (Part 1). https://www.woundsource.com/blog/understanding-braden-scale-focus-sensory-perception-part-1
Institute for Healthcare Improvement. (n.d.). What is a bundle? Retrieved April 21, 2022, from http://www.ihi.org/resources/Pages/ImprovementStories/WhatIsaBundle.aspx
Jackson, D., Sarki, A. M., Betteridge, R., & Brooke, J. (2019). Medical device-related pressure ulcers: A systematic review and meta-analysis. International Journal of Nursing Studies, 92, 109-120. https://doi.org/10.1016/j.ijnurstu.2019.02.006
Jmarchn. (2020). Pressure ulcer points [Image]. https://commons.wikimedia.org/wiki/File:Pressure_ulcer_points.svg
Johnson, C., Giordano, N. A., Patel, L., Book, K. A., Mac, J., Viscomi, J., Em, A., Westrick, A., Koganti, M., Tanpiengco, M., Sylvester, K., & Mastro, K. A. (2021). Pressure injury outcomes of a prone-positioning protocol in patients with COVID and ARDS. American Association of Critical-Care Nurses, 31(1), 34-41. https://doi.org/10.4037/ajcc2022242
The Joint Commission. (2018). Managing medical device-related pressure injuries. https://www.jointcommission.org/-/media/tjc/newsletters/qs_43_med_dev_pressure_injuries_7_17_18_final2pdf.pdf
The Joint Commission. (2022a). Hospital: 2022 national patient safety goals. https://www.jointcommission.org/standards/national-patient-safety-goals/hospital-national-patient-safety-goals
The Joint Commission. (2022b). Hospital acquired pressure ulcers/injuries (HAPU/I) prevention. https://www.centerfortransforminghealthcare.org/improvement-topics/hospital-acquired-pressure-ulcers-prevention/
Jones, J. & Williams, H. (2017). Wound management should not be a pain. Community Wound Care, 22(Suppl. 9), S38-S46. https://doi.org/10.12968/bjcn.2017.22.Sup9.S38
Kaur, A., Midha, S., Giri, S., & Mohanty, S. (2019). Functional skin grafts: Where biomaterials meet stem cells. Stem Cells International, 1-20. https://doi.org/10.1155/2019/1286054
Kim, P., Aribindi, V. K., Shui, A. M., Deshpande, S. S., Rangarajan, S., Schorger, K., Aldrich, M., & Lee, H. (2022). Risk factors for hospital-acquired pressure injury in adult critical care patients. American Journal of Critical Care, 31(1), 42-50. https://doi.org/10.4037/ajcc2022657
Kirman, C. N. (2020). Pressure injuries (pressure ulcers) and wound care. https://emedicine.medscape.com/article/190115-overview#a1
Manna, B., Nahirniak, P., & Morrison, C. A. (2021). Wound debridement. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK507882/
McCance, K. L., & Huether, S. E. (2019). Pathophysiology: The biologic basis for disease in adults and children (8th ed.). Elsevier.
Mechem, C. C., & Manaker, S. (2020). Hyperbaric oxygen therapy. UpToDate. Retrieved April 10, 2022, from https://www.uptodate.com/contents/hyperbaric-oxygen-therapy
Mennella, H., & Schub, E. (2018). Wound dressings: Foam – applying. CINAHL Nursing Guide. Retrieved April 19, 2022, from https://research.ebscomedical.com/eds/detail?db=nup&an=T704105
Miller, M. W., Emeny, R. T., Freed, G L. (2019). Reduction of hospital-acquired pressure injuries using a multidisciplinary team approach: A descriptive study. https://www.hmpgloballearningnetwork.com/site/wounds/article/reduction-hospital-acquired-pressure-injuries-using-multidisciplinary-team-approach
Mondragon, N., & Zito, P. M. (2021). Pressure injury. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK557868/
National Database of Nursing Quality Indicators. (2018). Admission skin and pressure injury risk assessment. https://members.nursingquality.org/ndnqipressureulcertraining/Module3/PressureULcerSurveyGuide_7.aspx
National Pressure Injury Advisory Panel. (n.d.). NPIAP pressure injury stages. Retrieved April 19, 2022, from https://cdn.ymaws.com/npiap.com/resource/resmgr/online_store/npiap_pressure_injury_stages.pdf
National Pressure Injury Advisory Panel. (2019). Prevention and treatment of pressure ulcers/injuries: Clinical practice guideline. https://www.biosanas.com.br/uploads/outros/artigos_cientificos/127/956e02196892d7140b9bb3cdf116d13b.pdf
Nelson, J. (2021). Antibiotics for wound infection. https://plushcare.com/blog/antibiotics-for-wound-infection/
Pilgrim, J., & Heering, H. (2017). Wound care: Sharp (surgical) debridement: Assisting with. CINAHL Nursing Guide. Retrieved April 19, 2022, from https://research.ebscomedical.com/eds/detail?db=nup&an=T706151
Schub, E., & Smith, N. (2021). Pressure injuries: Risk assessment and diagnosis. CINAHL Nursing Guide. Retrieved April 19, 2022, from https://research.ebscomedical.com/eds/detail?db=nup&an=T702548
Schub, E., & Walsh, K. (2018). Wound care: Performing maggot debridement therapy. CINAHL Nursing Guide. Retrieved April 19, 2022, from https://research.ebscomedical.com/eds/detail?db=nup&an=T706275
Singhal, H. (2021). Wound infection medication. https://emedicine.medscape.com/article/188988-medication#2
Smith, N., & Caple, C. (2019). Wound dressings: Hydrocolloid - applying. CINAHL Nursing Guide. Retrieved April 19, 2022, from https://research.ebscomedical.com/eds/detail?db=nup&an=T704120
Spinal Cord Injury Research Evidence. (n.d.). The Norton pressure sore risk-assessment scale scoring system. Retrieved April 18, 2022, from https://scireproject.com/wp-content/uploads/Norton_presure_sore_risk_assessment_scale.pdf
Walsh, K., & Schub, T. (2018). Wound dressings: Alginate absorptive – applying. CINAHL Nursing Guide. Retrieved April 19, 2022, from https://research.ebscomedical.com/eds/detail?db=nup&an=T704120
Weaver, P., Weaver, L., & Miller, C. (2021). Risk factors associated with medical device-related pressure injuries in the adult intensive care patient: a scoping review. Wound Practice & Research, 29(4), 219-225. https://doi.org/10.33235/wpr.29.4.219-225
Weber, P., Weaver, L., & Miller, C. (2021). Risk factors associated with medical device-related pressure injuries in the adult intensive care patient: a scoping review. Wound Practice and Research, 29(4), 219-225. https://doi.org/10.33235/wpr.29.4.219-225
Wernick, B., Nahirniak, P., & Stawicki, S. P. (2021). Impaired wound healing. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK482254/
Wood, B. (2021). Skin grafts and biologic skin substitutes. https://emedicine.medscape.com/article/1295109-overview